












4.0 Human Performance

Contents
- 4 HUMAN PERFORMANCE
- 4.1 Fitness-for-Duty Aerobic Capacity
- 4.2 Fitness-for-Duty Sensorimotor
- 4.3 Fitness-for-Duty Behavioral Health and Cognition
- 4.4 Fitness-for-Duty Hematology and Immunology
- 4.5 Permissible Outcome Limit for Nutrition
- 4.6 Permissible Outcome Limit for Muscle Strength
- 4.7 Permissible Outcome Limit for Microgravity-Induced Bone Mineral Density(BMD) Loss
- 4.8 Space Permissible Exposure Limit for Spaceflight Radiation Exposure
4 HUMAN PERFORMANCE
To support space exploration and to guide and focus efforts to protect the health of spacefaring crews, spaceflight health technical requirements for human performance have been developed. These technical requirements provide a declaration of acceptable medical risk from the deleterious health and performance effects of spaceflight and help target and prioritize biomedical research and technology development efforts, providing target parameters for products and deliverables that support the health maintenance of crews during space missions. They also promote operational and vehicle design technical requirements and aid in medical decision-making during space missions.
The technical requirements are based on the best available scientific and clinical evidence. Research findings, lessons learned from previous space missions and in analogue environments, current standards of medical practice, risk management data, and expert recommendations were all considered in the process of setting the technical requirements. The process used for setting the technical requirements was modeled on that used by the United States Occupational Safety and Health Administration (OSHA) but were tailored to meet the unique needs and characteristics associated with the human health aspects of space exploration and the NASA mission
4.1 Fitness-for-Duty Aerobic Capacity
An individual’s aerobic capacity influences the ability to perform a task at a given level of work. Aerobic capacity in conjunction with the operational concept provides an upper bound for oxygen (O2) demand. Aerobic capacity is determined by calculating VO2max which measures the maximum rate of oxygen a body can use during exercise/activity. Setting aerobic fitness for duty parameters is necessary to ensure the crew can perform required functions during all phases of spaceflight including extravehicular activities. Crew is provided with countermeasures enabling them to maintain their aerobic capacity throughout a mission including post-mission reconditioning.
4.1.1 Microgravity EVA Aerobic Capacity
[V1 4001] Crewmembers shall maintain an in-mission VO2max at or above 32.9 ml⁄min/kg for missions with microgravity EVAs as determined by either direct or indirect measures.
[Rationale: Expected EVA metabolic rates were determined based either on flight data or analog study data. The estimated microgravity data came from an unpublished database of Shuttle and ISS EVA metabolic rates and Neutral Buoyancy Laboratory (NBL) training metabolic rates. Data used for the ISS scenario were the flight metabolic data from Space Transportation System (STS)-114 through STS-135. These data were reported in kcal/hr and transferred into VO2 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔 using an assumed respiratory exchange ratio (RER) of 0.85 and a crewmember mass of 80 kg. The average duration of these EVAs was 6.67 hours with a maximum of 8 hours. Based on these numbers, the assumption that crewmembers would sustain 30% of their in-mission VO2max during EVA task performance was used to calculate the required in-mission VO2max minimum. Pre-mission recommendations are provided given the historical experience showing declines of 15-25% in VO2max but are not required as long as the in-mission VO2max of 32.9 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔 can be maintained. (See Table 4.1-1—Pre-mission VO2max Recommendations and Required Minimum Inmission VO2max.) This recommended in-mission VO2max would also be sufficient to address the average max EVA VO2, which was 19.4 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔, and even the average of the top 10 EVA max VO2 values, which was 32.3 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔.]
Table 4.1-1— Pre-mission VO2max Recommendations and Required Minimum In-mission
| Example Destination |
In-Mission VO2max |
Pre-Mission VO2max Recommendation (assuming an inmission 15% decline) |
Pre-mission VO2max Recommendation (assuming an inmission 25% decline) |
| ISS | 32.9 ml/ min/ kg | 38.7 ml/ min/ kg | 43.8 ml/ min/ kg |
4.1.2 Extraterrestrial Surface EVA Aerobic Capacity
[V1 4002] Crewmembers shall maintain an in-mission VO2max at or above 36.5 ml⁄min/kg for missions with extraterrestrial surface EVAs as determined by either direct or indirect measures.
[Rationale: Extraterrestrial Surface EVAs are determined to require additional aerobic capacity compared to microgravity EVAs. Currently there is no data to inform extraterrestrial aerobic capacity, therefore historical experience (Apollo and ISS) as well as analog and terrestrial studies are being used with the aim of developing aerobic fitness standards for exploration missions. For example, the Functional Mission Task Study (Sutterfield et al. 2019) contributed to the estimated extraterrestrial surface EVA aerobic limit by providing terrestrial data used to predict extraterrestrial EVA performance. Crewmembers completed simulated mission critical tasks (surface traverse and hill climb) following max VO2 cycling and rowing tests with conditions simulating ambulation during Lunar, Apollo missions, and ambulation in Mark III Space Suit Technology Demonstrator EVA Suit. Metabolic rates and max VO2 were measured and evaluated for ability to predict task performance. Use of logistic regression and Receiver Operating Characteristic (ROC) analyses revealed that as metabolic demands of tasks increased, fitness threshold increased. For example, the most restrictive conditions included having crewmembers complete simulated traverse in weighted spacesuits which elicited an approximate 3.5 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔 increase in VO2. This and similar data were considered as well as the terrestrial limit of 32.9 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔 (assuming ISS EVA working at 30-40% max aerobic capacity) to result in the current requirement of 36.5 𝑚𝑙 𝑚𝑖𝑛 ⁄ /𝑘𝑔. Further studies are taking place and will continue to inform these prediction numbers.]
4.1.3 In-Mission Aerobic Capacity
[V1 4003] The in-mission aerobic capacity shall be maintained, either through countermeasures or work performance, at or above 80% of the pre-mission capacity determined by either direct or indirect measures.
[Rationale: A relative permissible loss of aerobic capacity requirement was established as part of the maintenance of overall cardiovascular health. A decreased VO2max is a hallmark result of spaceflight and bedrest when conducted without application of effective countermeasures. Convertino et al. (1997) demonstrated a 6-16% reduction in VO2max after 10 days of bedrest and additional expected reductions during longer duration. The Cromwell et al. 2019 70-day bedrest study used mission-like ISS exercise equipment capability during long-duration bed rest as a spaceflight exercise analog and demonstrated improvements in VO2max and muscle power. The inmission ≥ 80% requirement was determined using historical (including ISS) and study data, see Scott. et al. (2023) Effects of exercise countermeasures on multisystem function in long duration spaceflight astronauts, that assumes average 15% decline in VO2max and showed decrements up to 20% do not impair mission objectives and can be reconditioned to pre-flight aerobic capacity during post-flight reconditioning. This is in addition to the performance-based aerobic capacity technical requirements [V1 4001] Microgravity EVA Aerobic Capacity and [V1 4002] Extraterrestrial Surface EVA Aerobic Capacity. Both the relative and performance-based requirements are to be considered when aerobic exercise countermeasure capabilities are included in space systems.]
4.1.4 Post-Mission Aerobic Capacity
[V1 4004] Post-mission reconditioning shall be aimed at achieving a VO2max at or above the crewmember’s pre-mission values.
[Rationale: Aerobic capacity can be decreased by approximately 10%–30% after spaceflight depending on duration and conditions (NASA Human Research Program [HRP] Evidence report HRP-047072). Crewmembers follow documented Crewmember medical requirements (per [V1 6009] Medical and Crew Health Technical Requirements Document), max VO2 is evaluated within 5-7 days of landing, and crewmembers are provided with a daily schedule of prescribed aerobic reconditioning exercises to enable them to return to pre-mission aerobic fitness. They are tested at pre-determined intervals to confirm reconditioning success.]
4.2 Fitness-for-Duty Sensorimotor
Sensorimotor functional capabilities include balance, locomotion, eye-hand coordination, gaze control, tactile perception, and spatial orientation. Crewmembers experience impacts to sensorimotor function during and following transitions in gravitational fields, such as during the launch and re-entry phases of spaceflight. These impacts can include vestibular dysfunction, motion sickness, spatial disorientation, and decrements in postural, locomotor, manual, and fine motor controls which can potentially result in impaired crew performance during launch, post-launch, landing and post-landing activities (e.g., capsule egress and EVAs). Sensorimotor function will be assessed throughout all aspects of the mission using metrics that are task specific. Countermeasures including pre- and in-flight training, post-landing assessments and reconditioning exercises, vehicle/system design, operational timelines, and pharmaceuticals will be provided to maintain sensorimotor function through all phases of flight including post-mission reconditioning. Requirements are written based on mission related activities and critical operations. For detailed discussions regarding the effects of spaceflight on sensorimotor/vestibular alterations, see chapter 5, Human Performance Capabilities, of the HIDH.
4.2.1 Pre-Mission Sensorimotor
[V1 4005] Pre-mission sensorimotor functioning shall be within normal clinical values for age and sex of the crewmember population.
4.2.2 In-Mission Fitness-for-Duty Sensorimotor
[V1 4006] In-mission Fitness-for-Duty technical requirements shall be guided by the nature of mission-associated critical operations (such as, but not limited to, vehicle control, robotic operations, and EVAs).
4.2.3 In-Mission Fitness-for-Duty Sensorimotor Metrics
[V1 4007] In-mission Fitness-for-Duty technical requirements shall be assessed using metrics that are task specific.
4.2.4 Sensorimotor Performance Limits
[V1 4008] Sensorimotor performance limits for each metric shall be operationally defined.
4.2.5 Sensorimotor Countermeasures
[V1 4009] Countermeasures shall maintain sensorimotor function within performance limits.
4.2.6 Post-Mission Sensorimotor Reconditioning
[V1 4010] Post-mission reconditioning shall be monitored and aimed at returning to baseline sensorimotor function.
4.3 Fitness-for-Duty Behavioral Health and Cognition
Cognitive capabilities include, but are not limited to, attention, memory, decision making, problem solving, logical reasoning, and spatial cognition that can impact both individual and/or team performance. Cognitive Workload is the user’s perceived level of time-stress, mental effort, and frustration required to complete a task. It is influenced by many factors, including task load, task scheduling, and task design. Perceived high or low workload can lead to crew hurrying, compromised performance, and increased crew stress, perceived low workload can lead to crew boredom, low attention, and high error rates. Workload Assessment tools such as the Bedford Scale or NASA Task Load Index are used to determine workload demands that result in optimal crew health and performance. Crew schedule will have established limits to ensure crew physical and psychosocial health and safety. It is important to recognize the significant role that physical activity/exercise plays in maintaining crew health and well-being. Crewmember behavioral, psychosocial, and cognitive state will be assessed and monitored through all mission phases to ensure they remain within clinically accepted values.
4.3.1 Mission Cognitive Status
[V1 4011] Pre-mission, in-mission, and post-mission crew behavioral health and crewmember cognitive status shall be within clinically accepted values as determined by behavioral health evaluations.
4.3.2 End-of-Mission Cognitive Assessment and Treatment
[V1 4012] End-of-mission assessment and treatment for crewmember cognitive status shall include cognitive assessment, monitoring, and as needed, transitioning the crewmember back to pre-mission values.
4.3.3 End-of-Mission Psychosocial Assessment
[V1 4013] End-of-mission assessment and treatment for behavioral health of the crewmember shall include behavioral health and psychosocial assessment, monitoring, and as needed, transitioning the crewmember back into terrestrial work, family, and society.
4.3.4 In-Mission Completion of Critical Tasks
[V1 4014] The planned number of hours for in-mission completion of critical tasks and events, workday, physical activity/exercise, and planned sleep period shall have established limits to assure continued crew health and safety.
4.4 Fitness-for-Duty Hematology and Immunology
The immunological status of crewmembers may be compromised by physiological effects associated with elevated levels of stress due to long-term habitation in a microgravity environment. Monitoring hematological and immunological function and providing countermeasures to help sustain hematologic and immunologic health is important to ensure crew health.
4.4.1 Pre-Mission Hematological/Immunological Function
[V1 4015] Crewmember pre-launch hematological/immunological function shall be within normative ranges established for the healthy general population.
4.4.2 In-Mission Hematological/Immunological Countermeasures
[V1 4016] In-mission countermeasures shall be in place to sustain hematological/immunological parameters within the normal range as determined by direct or indirect means.
4.4.3 Hematology and Immunology Countermeasures and Monitoring
[V1 4017] Countermeasures and monitoring shall ensure immune and hematology values remain outside the critical values, i.e., the level that represents a significant failure of the hematological/immunological system, and is associated with specific clinical morbidity, defined for specific parameters.
4.4.4 Post-Mission Hematological/Immunological
[V1 4018] Post-mission assessment and treatment shall be aimed at returning to pre-mission hematological/immunological baseline values.
4.5 Permissible Outcome Limit for Nutrition
Maintaining crewmember nutritional status is critical to support crew health and optimal crew performance during missions. Crewmember nutritional status is assessed and monitored over all mission phases. Crewmember nutritional needs are calculated based on individual age, sex, body mass, height, and activity factor, to determine crewmember intake. Countermeasures are provided including prescribed diet and supplements, if necessary, to ensure that crewmembers have adequate nutritional intake and nutrients.
4.5.1 Pre-Mission Nutritional Status
[V1 4019] Pre-mission nutritional status shall be assessed, and any deficiencies mitigated prior to launch.
4.5.2 In-Mission Nutrient Intake
[V1 4020] Programs shall provide each crewmember with 100% of their calculated nutrient and energy requirements, based on an individual’s age, sex, body mass (kg), height (m), and appropriate activity factor.
4.5.3 Post-Mission Nutritional Assessment and Treatment
[V1 4022] Post-mission nutritional assessment and treatment shall be aimed at returning to premission baseline.
4.6 Permissible Outcome Limit for Muscle Strength
Skeletal muscle is essential to human health and functional performance as both a contractile tissue responsible for force production and a highly metabolic tissue influencing energy balance. Microgravity environments encountered in space travel can result in a loss of muscle mass and muscle strength. Maintaining adequate strength levels is essential for effective performance of spaceflight tasks, emergency egress from a vehicle, and general function upon return to Earth. Deconditioned crewmembers may be at increased risk for falls and difficulty with assigned tasks and activities of daily living upon return. Pre-mission muscle strength and function requirements are designed to provide sufficient strength to complete in-flight and post-flight tasks, while maintaining operational efficiency and preserving muscle strength for off-nominal events. Countermeasures such as exercise devices are provided through all phases of a mission to maintain skeletal muscle strength.
4.6.1 Pre-Mission Muscle Strength and Function
[V1 4023] Pre-mission muscle strength and function shall meet or exceed the values in Table 4.6- 1—Pre-Mission Muscle Strength.
[Rationale: Crewmember strength capacity is to be sufficient to complete in-flight and post-flight nominal tasks, maintain operational efficiency, minimize loss of mission objectives, and unaided egress. Table 4.6-1—Pre-Mission Muscle Strength Requirements, provides strength standards for missions with microgravity EVAs, extraterrestrial surface EVAs, and unaided egress. It may be possible for crewmembers who fall below these standards to complete tasks, however it could require additional time and resources. EVA suit design (i.e., suit design impacts the ability of the human to perform) needs to be considered and may require adjustment to the values. The bodyweight metric for lower body strength (i.e., deadlift) is used in the Army Combat Fitness Testing battery and was identified as a generalizable measurement. The lower body strength standard for unaided egress is consistent with a calculated strength threshold using a previously published relationship between isometric midthigh pull and deadlift (De Witt et al. 2018) along with midthigh pull data collected during simulated space exploration tasks (Ryder 2019). The metric for upper body strength (i.e., bench press) is based on values reported in military populations and also utilizing data from Ryder 2019.]
Table 4.6-1—Pre-Mission Muscle Strength
| Minimum | Microgravity EVAs |
Extraterrestrial Surface EVAs | Unaided Terrestrial Egress |
|
|---|---|---|---|---|
| Deadlift | 1.0 x Body Weight | 1.3 x Body Weight | 1.6 x Body Weight | 1.3 x Body Weight |
| Bench Press | 0.7 x Body Weight | 0.8 x Body Weight | 1.0 x Body Weight | 0.7 x Body Weight |
4.6.2 In-Mission Skeletal Muscle Strength
[V1 4024] Countermeasures shall maintain in-mission skeletal muscle strength at or above 80% of baseline values.
[Rationale: A relative permissible loss of muscle strength standard was established for maintenance of overall musculoskeletal heath. The Cromwell et al 2019 70-day bedrest study used mission-like ISS exercise equipment capability during long-duration bed rest as spaceflight exercise analog and demonstrated improvements in VO2max and muscle power. The 80% minimum was determined using historical (including ISS) study data showing decrements up to 20% do not impair mission objectives and can be reconditioned to pre-flight muscular strength during post-flight reconditioning (NASA Human Research Program HRP-47072 Evidence Report: Risk of Impaired Performance Due to Reduced Muscle Mass, Strength, and Endurance). This requirement is in addition to the performance-based requirement [V1 4023] Pre-Mission Muscle Strength and Function. Both the relative and performance-based requirements are to be considered when resistance exercise countermeasure capabilities are included in space systems.]
4.6.3 Post-Mission Muscle Reconditioning
[V1 4025] Post-mission reconditioning shall be aimed at returning to baseline muscle strength.
[Rationale: Lower body muscle cross-sectional area and strength can be decreased by approximately 10–30% after spaceflight depending on duration and conditions (NASA Human Research Program HRP-47072) Evidence Report: Risk of Impaired Performance Due to Reduced Muscle Mass, Strength, and Endurance). Crewmembers follow program reconditioning guidelines, (per [V1 6009] Medical and Crew Health Technical Requirements Document)); strength is evaluated within 5-7 days of landing, and crewmembers are provided with a daily schedule of prescribed aerobic and strength reconditioning exercises, to enable them to return to pre-mission strength. They are tested at pre-determined intervals to confirm reconditioning success. Further studies are taking place and will continue to inform these prediction numbers.]
4.7 Permissible Outcome Limit for Microgravity-Induced Bone Mineral Density(BMD) Loss
Crewmembers experience decrements in bone mineral density (BMD) during long-duration spaceflight. These changes are concerning due to increased susceptibility to fracture when an external load or unexpected load is applied. These risks could be elevated for longer duration spaceflights where crewmembers may be exposed to microgravity for more than a year. Additional concern is the fact that not all the BMD lost during spaceflight is regained, increasing risk for early onset osteoporosis and fracture risk later in life. Uncertainty still exists regarding changes during spaceflight in BMD, bone structure, and bone microarchitecture, and how these changes might influence fracture risk. In addition to the loss of bone mineral density, it’s worth noting that hypercalciuria associated with perturbed bone remodeling can also contribute to the risk of developing renal stones. This is particularly important to consider as the mission impact of renal stones may be higher than that of the BMD loss alone. Changes in bone mineral density with spaceflight and with aging have been well characterized in the crewmember cohort. Longitudinal monitoring of BMD is utilized to assess declines in response to in-flight countermeasures such as exercise and pharmaceuticals.
4.7.1 Pre-Mission Bone Mineral Density
[V1 4026] Crewmembers’ pre-mission bone mineral density (BMD) T-scores for total hip and lumbar spine (L1-L4), as measured by mass dual energy X-ray absorptiometry (DXA) shall be consistent with an age, sex, gender, and ethnic-matched population.
4.7.2 In-Mission Bone Countermeasures
[V1 4027] Countermeasures shall maintain bone mineral density of the hip and spine at or above 95% of pre-mission values and at or above 90% for the femoral neck.
[Rationale: Countermeasures, including an advanced resistive exercise device (ARED), cycle ergometer device, and treadmill, have resulted in the majority of crewmembers returning with <10% deficit bone mineral density in femoral neck and <5% in total hip or spine during 6-month ISS missions. Additional countermeasures may also include pharmacological antiresorptive (bisphosphonate) therapy which has been tested in research space studies and decreased the bone loss further (~0% loss) when used in combination with exercise countermeasures. Post-mission long-term effects to bone health are being monitored.]
4.7.3 Post-Mission Bone Reconditioning
[V1 4028] Post-mission reconditioning shall be aimed at returning bone mineral density to premission baseline values.
4.8 Space Permissible Exposure Limit for Spaceflight Radiation Exposure
The following technical requirements define the Space Permissible Exposure Limits (PELs) for the following: crewmember total career exposure limits, short-term acute exposure limits, and nuclear technology exposure limits. It is important to further minimize exposure from all sources of radiation below the following limits using the As Low As Reasonably Achievable (ALARA) principle. Refer to NASA-STD-3001 Volume 2 section 6.8.1 Ionizing Radiation for vehicle design technical requirements.
4.8.1 As Low as Reasonably Achievable (ALARA) Principle
[V1 4029] All crewmember radiation exposures shall be minimized using the ALARA principle.
[Rationale: It is important to minimize crewmember health risk due to radiation exposure by decreasing crewmember radiation exposure from all sources using the ALARA principle. The ALARA principle is a fundamental guiding principle for radiation protection which requires programs to minimize radiation exposures below the limits/technical requirements within the design constraints of the mission.]
4.8.2 Career Space Permissible Exposure Limit for Spaceflight Radiation
[V1 4030] An individual crewmember’s total career effective radiation dose due to spaceflight radiation exposure shall be less than 600 mSv. This limit is universal for all ages and sexes.
Note: The NASA effective dose for determining the threshold limit is calculated using the NASA Q (based on the NASA cancer model of 2012 as referenced in Human Health and Performance Risks of Space Exploration Missions Evidence Book 2009), 35-year-old female model parameters (tissue weighting factors, phantom etc.), for both males and females. Individual crewmember REID calculations are calculated using the appropriate NASA Q (based on the NASA cancer model of 2012) sex and age model parameters.
[Rationale: For background on setting the limit for this standard, refer to National Academies of Sciences, Engineering, and Medicine 2021. Space Radiation and Astronaut Health: Managing and Communicating Cancer Risks. Washington, DC: The National Academies Press. https://doi.org/10.17226/26155. The total career dose limit is based on ensuring each crewmember (inclusive of all ages and sexes) remains below 3% mean risk of cancer mortality (risk of exposure-induced death (REID)) above the non-exposed baseline mean. 3% was chosen due to being in the family of individual lifestyle changes (e.g., smoking, lack of exercise). Individual crewmember career dose includes all past spaceflight radiation exposures, plus the projected exposure for an upcoming mission. Medical and biomedical research exposures are not included in the dose limit but are tracked for overall crewmember exposure history. This technical requirement protects the career limits for all organs in Table 4.8-1—Dose Limits for Career/Non-Career Effects (in mGy-Eq or mGy), and Table 4.8-2—Relative Biological Effectiveness (RBE) for Non-Cancer Effects of the Lens, Skin, BFO, and Circulatory Systems, using mGy-eq calculations. All crewmember radiation exposures are to be minimized using the ALARA principle as referenced in [V1 4029] As Low as Reasonably Achievable (ALARA). Due to variability and subjectivity of the selection of model parameters that can easily modify the model output by 25%,, the model need not be updated unless new data indicates a 30% change is seen in the effective dose associated with the 3% mean REID calculation. Refer to NASA/TP-2020-5008710, Ensemble Methodologies for Astronaut Cancer Risk Assessment in the face of Large Uncertainties.]
Table 4.8-1—Dose Limits for Career/Non-Cancer Effects (in mGy-Eq. or mGy)
Note: RBEs for specific risks are distinct as described below.
| Organ | 30-DayLlimit | 1-Year Limit | Career |
|---|---|---|---|
| Lens*# | 1,000 mGy-Eq | 2,000 mGy-Eq | 4,000 mGy-Eq |
| Skin# | 1,500 mGy-Eq | 3,000 mGy-Eq | 6,000 mGy-Eq |
| Blood-forming Organs# | 250 mGy-Eq | 500 mGy-Eq | Not applicable |
| Circulatory System**## | 250 mGy-Eq | 500 mGy-Eq | 1000 mGy-Eq |
| Central Nervous System***## | 500 mGy | 1,000 mGy | 1,500 mGy |
| Central Nervous System*** (Z≥10)## | – | 100 mGy | 250 mGy |
| *Lens limits are intended to prevent early (<5 years) severe cataracts, e.g., from a solar particle event. An additional cataract risk exists at lower doses from cosmic rays for sub-clinical cataracts, which may progress to severe types after long latency (>5 years) and are not preventable by existing mitigation measures; however, they are deemed an acceptable risk to the program. **Circulatory system doses calculated as average over heart muscle and adjacent arteries. ***Central Nervous System limits are to be calculated at the hippocampus. Reference: National Council on Radiation Protection and Measurements. 2000. Recommendations of Dose Limits for Low Earth Orbit. NCRP Report 132, Bethesda MD. Human Research Program Evidence Book 2009. Human Research Program Space Radiation Program Element Risk Evidence book of Acute and Late Central Nervous System Effects from Radiation Exposure 2016 |
4.8.3 Radiation Limits – Solar Particle Events
[V1 4031] The program shall protect crewmembers from exposure to the design reference Solar Particle Event (SPE) environment proton energy spectrum (sum of the October 1989 events) to less than an effective dose of 250 mSv.
[Rationale: The 250 mSv effective dose threshold was chosen to minimize acute effects and protects for the limits for all organs listed in Table 4.8-1 Dose Limits for Career/Non-Cancer Effects (in mGy-Eq. or mGy). In the design process, ALARA ensures optimization of the design to afford the most protection possible within other constraints of the vehicle systems. The additional protection significantly contributes to the mitigation of long-term health effects such as cancer (refer to [V1 4030] Career Space Permissible Exposure Limit for Spaceflight Radiation).
Table 4.8-3 contains the Design Reference SPE Environment Proton Energy Spectrum. SPE shielding is to be an inherent part of the vehicle design and/or reconfigured components within the vehicle to minimize the addition of mass. To be most effective, it is critical that the shielding surrounds the crew. The design solution which includes considerations for the vehicle/habitat needs to minimize exposure as much as possible utilizing the ALARA principle. For SPE shielding designs, an iterative approach is to be taken for determining shielding designs that continue to iterate the design until less than a 10 mSv is achieved from the previous iteration. If a reconfigurable shelter is deployed, Environmental Control Life Support System (ECLSS) impacts need to be considered. Refer to Table 4.8-4—Recommended Shielding Guidelines for SPEs, for shielding recommendations based on mission duration and location.]
Table 4.8-3—Design Reference SPE Environment Proton Energy Spectrum (Sum of the
October 1989 Events)
| Energy | Proton Fluence | Energy | Proton Fluence | Energy | Proton Fluence | Energy | Proton Fluence | Energy | Proton Fluence |
| (MeV) | (#/cm2-MeV) | (MeV) | (#/cm2-MeV) | (MeV) | (#/cm2-MeV) | (MeV) | (#/cm2-MeV) | (MeV) | (#/cm2-MeV) |
| 1.000E-02 | 7.761E+14 | 7.761E+14 | 3.651E+11 | 4.810E+00 | 9.004E+09 | 3.426E+01 | 1.641E+08 | 2.484E+02 | 5.714E+05 |
| 1.338E-02 | 4.329E+14 | 6.480E-01 | 2.979E+11 | 5.317E+00 | 7.510E+09 | 3.775E+01 | 1.298E+08 | 2.756E+02 | 4.006E+05 |
| 1.790E-02 | 2.424E+14 | 7.263E-01 | 2.442E+11 | 5.875E+00 | 6.257E+09 | 4.160E+01 | 1.022E+08 | 3.060E+02 | 2.773E+05 |
| 2.391E-02 | 1.369E+14 | 8.129E-01 | 2.008E+11 | 6.490E+00 | 5.208E+09 | 4.584E+01 | 8.008E+07 | 3.407E+02 | 1.862E+05 |
| 3.183E-02 | 7.805E+13 | 9.086E-01 | 1.655E+11 | 7.168E+00 | 4.330E+09 | 5.052E+01 | 6.136E+07 | 3.794E+02 | 1.230E+05 |
| 4.210E-02 | 4.531E+13 | 1.014E+00 | 1.368E+11 | 7.914E+00 | 3.594E+09 | 5.568E+01 | 4.700E+07 | 4.232E+02 | 8.060E+04 |
| 5.511E-02 | 2.697E+13 | 1.130E+00 | 1.135E+11 | 8.736E+00 | 2.979E+09 | 6.137E+01 | 3.600E+07 | 4.728E+02 | 5.236E+04 |
| 7.112E-02 | 1.657E+13 | 1.258E+00 | 9.421E+10 | 9.641E+00 | 2.465E+09 | 6.765E+01 | 2.754E+07 | 5.291E+02 | 3.367E+04 |
| 9.027E-02 | 1.055E+13 | 1.400E+00 | 7.839E+10 | 1.064E+01 | 2.035E+09 | 7.460E+01 | 2.103E+07 | 5.930E+02 | 2.141E+04 |
| 1.125E-01 | 6.989E+12 | 1.556E+00 | 6.527E+10 | 1.174E+01 | 1.677E+09 | 8.226E+01 | 1.603E+07 | 6.665E+02 | 1.337E+04 |
| 1.375E-01 | 4.810E+12 | 1.729E+00 | 5.441E+10 | 1.294E+01 | 1.379E+09 | 9.074E+01 | 1.219E+07 | 7.505E+02 | 8.141E+03 |
| 1.657E-01 | 3.411E+12 | 1.919E+00 | 4.541E+10 | 1.427E+01 | 1.131E+09 | 1.001E+02 | 9.237E+06 | 8.471E+02 | 4.859E+03 |
| 1.968E-01 | 2.489E+12 | 2.129E+00 | 3.792E+10 | 1.574E+01 | 9.248E+08 | 1.105E+02 | 6.966E+06 | 9.588E+02 | 2.856E+03 |
| 2.303E-01 | 1.872E+12 | 2.361E+00 | 3.168E+10 | 1.735E+01 | 7.542E+08 | 1.220E+02 | 5.234E+06 | 1.091E+03 | 1.633E+03 |
| 2.675E-01 | 1.428E+12 | 2.617E+00 | 2.647E+10 | 1.913E+01 | 6.132E+08 | 1.348E+02 | 3.908E+06 | 1.244E+03 | 9.199E+02 |
| 3.082E-01 | 1.108E+12 | 2.900E+00 | 2.213E+10 | 2.108E+01 | 4.969E+08 | 1.490E+02 | 2.902E+06 | 1.418E+03 | 5.152E+02 |
| 3.525E-01 | 8.711E+11 | 3.211E+00 | 1.850E+10 | 2.323E+01 | 4.013E+08 | 1.648E+02 | 2.134E+06 | 1.625E+03 | 2.802E+02 |
| 4.010E-01 | 6.929E+11 | 3.555E+00 | 1.546E+10 | 2.561E+01 | 3.229E+08 | 1.824E+02 | 1.560E+06 | 1.869E+03 | 1.486E+02 |
| 4.542E-01 | 5.560E+11 | 3.933E+00 | 1.292E+10 | 2.822E+01 | 2.588E+08 | 2.018E+02 | 1.131E+06 | 2.158E+03 | 7.696E+01 |
| 5.126E-01 | 4.493E+11 | 4.350E+00 | 1.079E+10 | 3.109E+01 | 2.065E+08 | 2.239E+02 | 8.074E+05 | 2.500E+03 | 3.891E+01 |
Table 4.8-4—Recommended Shielding Guidelines for SPEs
| Mission Location and Duration | Shielding* | Type(s) of Shielding | Comments |
| Celestial surface, any duration | 10 cm (or g/cm2) water equivalent surrounding the crewmember. Considers celestial surface shielding contribution | Reconfigurable shielding already within the vehicle | Timeline of SPEs allows for reconfiguration |
| Beyond low earth orbit <6 months | 15 cm (or g/cm2) water equivalent surrounding the crewmember | Reconfigurable shielding already within the vehicle. Shielding may include personal protective equipment (PPE) | Timeline of SPEs allows for reconfiguration |
| Beyond low earth orbit > 6 Months | 20 cm (or g/cm2) water equivalent surrounding the crewmember | Integrated vehicle and/or reconfigurable Shielding which may include PPE | Long duration missions increase the probability of the crew being exposed SPEs |
| *The shielding required to meet the technical requirement (utilizing existing mass when feasible). |
4.8.4 Crew Radiation Limits for Nuclear Technologies
[V1 4032] Radiological exposure from nuclear technologies emitting ionizing radiation to crewmembers (e.g., radioisotope power systems, fission reactors, etc.) shall be less than an effective dose of 20 mSv per mission year (prorated/extrapolated to mission durations) utilizing the ALARA principle.
[Rationale: This limit is based on adding no more than 10% radiation exposure beyond the space environment radiation of the mission. Based on an analysis for a surface-based mission (see Figure 4.8-1 Ronald E. Turner (2022) Impact of Solar Cycle Duration on Astronaut Radiation Exposure during a Human Mars Mission), the radiation environment exposure is approximately 0.5 mSv per day; and 10% of this value sets the technical requirement to 0.05 mSv per day and ~20 mSv/mission year. This technical requirement is applied to both surface and free-space missions regardless of mission solar cycle. 20 mSv is also based on the occupational workers limit guideline from the ICRP, (The 2007 Recommendations of the International Commission on Radiological Protection, ICRP 103, 2007).
For a typical surface power application, the allowable crewmember dose can be converted to an effective reactor dose for shield sizing. The effective reactor dose would be calculated by estimating the time a crewmember spends in a shielded habitat versus the time spent during unshielded EVAs over a typical mission timeline. Exact mission assumptions need to be considered when performing the calculation; parameters are to include estimates of time in a habitat, habitat shielding, and EVA frequency. Example parameters to be considered: time fraction (67%) in the habitat, habitat shielding (20 g/cm2), terrain shielding, distance from source, line of sight to source, and time fraction (33%) of performing EVAs.
Space radiation and radioactive source tradeoff for a waiver of technical requirement consideration: For missions that are leveraging nuclear sources for a propulsion system, the tradeoff of reduced mission duration due to faster transit, which reduces the crew exposure to spaceflight radiation, is to be considered compared to the increased exposure due to the nuclear source. For example, if the nuclear propulsion system saves 90 days of exposure over a one year transit to Mars (which equates to 1.5 mSv/day × 90 days = 135 mSv “saved” spaceflight radiation exposure) and the source generates 150 mSv, then the net exposure is +15 mSv. Other considerations for reduced mission time on engineering risks (systems reliability, logistics, etc.) and other human risks such as bone loss, renal stone development, and medical care is to be considered in the waiver process.]
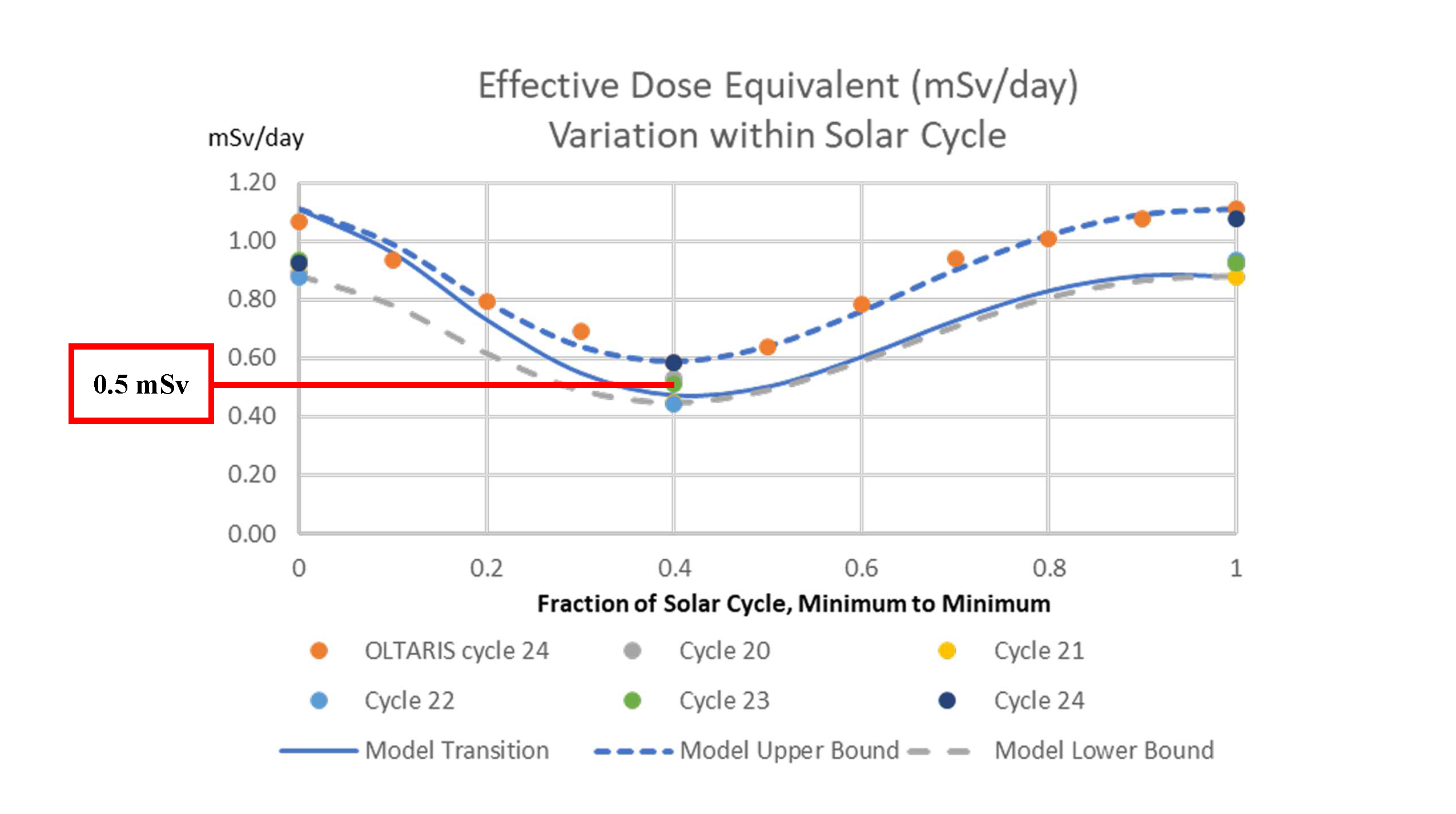
Figure 4.8-1—Effective Dose (mSv per Mission Day) Variation with Solar Cycle
4.8.5 Crew Radiation Limits from Galactic Cosmic Radiation
[V1 4033] For habitable space systems designed to support crew for > 60 days, the program shall protect crewmembers from exposure to the galactic cosmic ray (GCR) environment to less than a NASA effective dose (as defined in NASA-STD-3001, Volume 1 [V1 4030] Career Space Permissible Exposure Limits for Spaceflight Radiation) rate of 1.3 mSv/day for systems in free space and to less than 0.9 mSv/day for systems on planetary surfaces.
Note: To verify the habitable space system design meets the GCR protection requirement above, the NASA effective dose rate is calculated using the 2009 solar minimum Badhwar O’Neill GCR model spectrum and take into account estimated crew time spent at lightly and more heavily shielded locations throughout the habitable space system. If achievable, further measures are to be taken to reduce crew exposure in accordance with the ALARA principle, as set forth in [V1 4029] As Low as Reasonably Achievable (ALARA) Principle.
[Rationale: This requirement applies to missions beyond Low-Earth orbit. For these missions, vehicle and habitat systems need to be designed to provide sufficient protection to reduce exposure from GCR by at least 15% in free space and by at least 10% on the lunar surface. The 60-day minimum is designated to protect crewmembers beyond short duration initial capability missions. This ensures risks are minimized while maximizing spaceflight opportunities for crewmembers within the limits set forth in [V1 4029] As Low as Reasonably Achievable (ALARA) Principle and [V1 4030] Career Space Permissible Exposure Limits for Spaceflight Radiation. The design reference environment is the 2009 solar minimum spectrum as described by the Badhwar O’Neill 2020 GCR Model. During solar minimum, vehicle shielding can effectively reduce the free space, unshielded GCR effective dose rate of 1.5 mSv/day by approximately 15% to 1.3 mSv/day or lower depending on the vehicle/shielding materials incorporated into vehicle design. While shielding against the build-up of secondary neutrons on the lunar surface is more challenging, reductions of 10% can be effectively realized for lunar surface systems. Reductions can be achieved with shielding density thickness between 10-40 g/cm2 . Further reductions to effective dose are difficult to realize given the fact that shield density thickness between 40-100 g/cm2 have either a negligible or negative impact on the exposure rate, while potentially introducing a significant mass/launch burden. Additional shielding on the Mars surface is likely not beneficial unless hydrogenous materials are incorporated for long duration stays.]