



















“Houston We Have a Podcast” is the official podcast of the NASA Johnson Space Center, the home of human spaceflight, stationed in Houston, Texas. We bring space right to you! On this podcast, you’ll learn from some of the brightest minds of America’s space agency as they discuss topics in engineering, science, technology and more. You’ll hear firsthand from astronauts what it’s like to launch atop a rocket, live in space and re-enter the Earth’s atmosphere. And you’ll listen in to the more human side of space as our guests tell stories of behind-the-scenes moments never heard before.
Dr. Lucie Low, Scientific Program Manager at the National Institutes of Health, talks about tiny devices the size of the thumb drive that replicate the structure and function of human organs. Low discusses the importance of testing these devices in space. This episode was recorded on September 25, 2018.
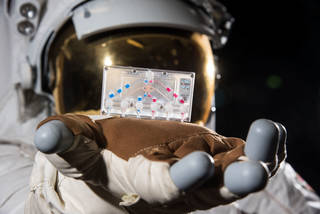
Check out “Small Tissue Chips in Space a Big Leap Forward for Research” to learn more about these chips.

Transcript
Gary Jordan (Host): Houston, We Have a Podcast. Welcome to the official podcast of the NASA Johnson Space Center, Episode 70: Organs on Chips in Space. I’m Gary Jordan, and I’ll be your host today. On this podcast, we bring in the experts, NASA scientists, engineers, and astronauts all to let you know the coolest information about what’s going on in America’s space agency. So, the International Space Station is a lab, a big one in space. And one of the greatest opportunities presented by this lab is the ability to test things in microgravity. We have a lot of tests focused at looking at the human body, because a lot happens in this unique environment, muscle deteriorate, bones resemble signs of osteoporosis, and humans seem to age faster. We figured out ways to counteract these effects, even reverse them, but there’s still so much to learn. Because there are so many parts of the human body. But what if you can isolate organs, cells and tissues and really get a look at what’s going on? Well, there’s a way to do that with science and it’s weird. So, today we’re talking with Lucie Low. She’s the scientific program manager for the Trans-NIH Tissue Chip for Drug Screening Program for the National Center for Advancing Translational Sciences, NCATS at that National Institutes of Health, NIH. They’ve partnered with CASIS. The organization that manages the national lab on the Space Station to send up what are called Tissue Chips, basically devices the size of a thumb drive and they have living human tissues and cells in them. They’re these little clear chips that are designed to be accurate models of the structure and functions of human organs like the lung, the liver, and the heart. Yeah, I know, straight-up sci-fi but it’s real and it’s happening aboard the International Space Station. So with no further delay, let’s have Dr. Lucie Low tell us about these little chips and what they’re doing in space, and what they aim to discover. Enjoy.
[ Music ]
Host: Lucie, thank you so much for coming on the podcast today to describe this weird tissue chip thing. I don’t even know where to begin with this stuff.
Dr. Lucie Low: It is straight-up sci-fi. I mean, straight-up sci-fi.
Host: So, organs, organs on chips. I don’t understand how this—why don’t we just kind of start with just, what is it?
Dr. Lucie Low: Okay.
Host: We’re talking about tissues chips, let’s just start with that. What is a tissue chip?
Dr. Lucie Low: Okay, so a tissue chip or an organ on a chip, its official fancy name is a Microphysical System or MPS and it is essentially a small bioreactor if you like. It’s a bioengineered micro device that contains human cells, it could be animal cells, but we focus on human cells, in a 3-dimenstional cultural system in some kind of scaffold. So, it’s essentially kind of recreating, recapitulating human tissues in this bioengineered bioreactor. And so, a tissue chip we say that we have three main properties that actually constitutes a tissue chip. We say that it has to be 3-dimensional, otherwise it’s just a flat layer of cells on a plate and humans are 3-dimensional. They’re not 2-dimensional. So we need something that’s 3-dimensional. We also want multiple different kinds of cell types. So, your liver for example is not just made up of hepatocytes or liver cells, it’s made up of all kinds of endothelial cells, connective tissues, immune tissues, all that kind of good stuff. So, we want multiple different kinds of tissue types within our tissue chip and then we also supply fluids to it by microfluidic channels for example, and the idea here is that every single tissue in your body has microvasculature and vasculature associated with it, it has to bring blood, it has to bring fluids, it has to bring nutrients, and it has to take away all the detritus that your cells create, all the rubbish that comes out of your cells has to get flown away.
So, that is how microfluidics comes into it, because you are then not only providing a means of support for the tissues with all of the stuff that you’re sending to them, but you’re also subjecting them to a lot of the kinds of stretch and shear forces that all of your tissues are subject to in vivo every single day. So, if you think about your lungs, they don’t just sit there. They stretch, they expand and then they contract. Every single cell in your lung is there for expanding and contracting every single day, multiple different times. So, the idea is that tissue chips can model these kinds of stretches, these kinds of shear forces, this kind of pulsatile flow as you get blood pumping through the system, exposure to all these different kinds of cell types, exposure to some kind of immune response and it’s all in this tiny little system that could be the size of a USB stick.
Host: Wow. That’s how big they are? You’re jamming this all into something that’s the size of a USB stick?
Dr. Lucie Low: So, the small ones can be really small. They could be the size of the modern futuristic USB sticks. Some of the other ones might be a bit bigger, especially if you are talking about which we can talk about later, is linked-organ systems.
Host: Yeah.
Dr. Lucie Low: You might get something bigger. The size of a modern day petri dish.
Host: Okay. Okay. So, how do you, is you’re talking about all these different complicated systems, Is this, are all of these in one single tissue chip or are they connected and simulating them individually?
Dr. Lucie Low: So, that’s a great question. So, the tissue chip field has really evolved and exploded over the past few years, and as a result of that, there’s this massive diversity in the systems that we have. So, you might have one single chip that’s quite straightforward, it’s just modeling say one single tissue and there might be other chips that model other single tissues and then there’s ways to link those physically through pumps and through microfluidic channels, or you might get systems that on one single plate have multiple different sort of pots for your different kinds of tissues and then you can perfuse those with what’s called, we would call a universal medium or a blood memetic. So, you could get multiple different kinds of tissues within one system, and so there’s really a broad range of everything from single tissues to multiple linked tissues. The linked tissues is harder. It’s much more complicated for a number of reasons, but it definitely starts off with one single tissue and then you can build from that.
Host: Okay. So, how does, how does it work? When you say tissue chip what I’m imaging is a heart in like something that’s a chip, but I don’t think that’s what it is.
Dr. Lucie Low: So, the “chips” word comes from the idea that the original chips were made often with silicon plastics much like computer chips, processor chips. So, that’s where that idea came from and the idea of this micro-embossing and microfluidics and micro technology is where that kind of concept of computer chips to tissue chips came from. But nowadays, there’s such a, like I said, this huge broad diversity in these different kinds of systems that really the key concept of what a tissue chip is, is this space, this pot, this bioreactor where you can chuck in a bunch of different cells from a number of different sources and we can talk a bit more about some of the challenges faced with cell sourcing for example, but essentially you throw all these cells together, you provide them with the nutrients they need, they buzz along and they do their thing and they chitchat to each other, and then what you get is a functional unit of what human tissues are like in vitro is the key thing; it’s outside of your body. So, it’s literally like taking a little bit of you and putting it into a pot, letting the cells chat to each other, looking at how they respond to different stresses, different drugs, different genetics, and then seeing what they do in vitro to predict what your body is doing in vivo.
Host: Huh, okay. So, it’s not necessarily a tiny heart in the chip. It’s all the components of the heart working together, getting the nutrients it needs and then you do what to it to say, to understand how it reacts? Are you putting drugs in there? Are you, what are you doing to it?
Dr. Lucie Low: Exactly. So, let’s look at the heart as an example.
Host: Yes.
Dr. Lucie Low: So, your heart isn’t just one amorphous blob. It might look like it from the outside, but it’s incredibly complicated.
Host: Oh yeah.
Dr. Lucie Low: You have different kinds of cardiomyocytes or heart cells in the atria as you do in the ventricles, and so the cardiomyocytes that makeup that blob of tissue that you’re working to make it a tissue chip are going to be slightly different. So, it might be that some researchers decided to focus on the atrium. So, they’ll look at atrial cardiomyocytes. They might decide to look at atrial fibrillation, so they might be able to take some kinds of skin cells, for example, fibroblasts from patients with atrial fibrillation. They can do what’s called or use stem cell technology and create induced pluripotent stem cell derived cells from these people’s skin cells and create small blobs of atrial tissue that is derived from that person who’s got atrial fibrillation.
Host: Okay.
Dr. Lucie Low: In this in vivo—in vitro system. Then they can start looking at the effects of different drugs. They can start looking at the effects of different stresses, different carbon dioxide levels All kinds of different things. They can start if they want to get really fancy, is they can start looking at the effect of gene editing techniques on these tissues to see how they’ll then respond in vitro to be able to predict what human responses would be.
Host: Okay. So, you can even isolate specific functions of the complicated organ and say—
Dr. Lucie Low: Yeah.
Host: I want to know what this does to this specific thing whenever this stimulus, this drug, this whatever is applied?
Dr. Lucie Low: Exactly. Exactly.
Host: Okay.
Dr. Lucie Low: And so, tissue chips have this really broad range of potential functionalities. So, they arose because there was a need in the drug development process to have better predicted models of human physiology. So, right now through the drug development process, there is this huge attrition rate. The number of drugs that get approved is exponentially tiny compared to the number of molecules that might be potential hits in lead compounds during that development process. And there’s a few reasons for that and a couple of those reasons are firstly that many of the molecules that get put, that come out of drug development processes turn out to be toxic. They might be toxic to cells on a 2-dimensional level. They might be toxic in animals, or worse, they might be toxic when you put them into human subjects in early clinical trials. Now, that’s a big no-no and that’s what we want to avoid.
Host: Yeah.
Dr. Lucie Low: Another reason that a lot of drugs fail is because they don’t actually do what they’re supposed to be doing. This is a concept of efficacy. So, you can run a bunch of tests in vitro in a 2-dimensional well plate. You can run a bunch of tests in animals which provide a wonderful analog of a whole organism system, but animals are not humans. Humans are animals, but that’s a different discussion. [laughter] The idea is that animal and human physiology can be very different. We have different ways of metabolizing drugs in our liver, all kinds of different enzymes and so there’s a real disconnect between all these wonderful drugs that are coming out that are actually going to be useful. And so, tissue chips actually arose as a way to be able to understand human physiology to be able to gauge toxicity much earlier on in the drug development process. And then to be able to check that potentially some of the drugs that are coming through that pipeline are actually going to be doing what they’re supposed to be doing without some necessary, or necessarily adverse side effects.
Host: Uh-hum. Without actually giving it to a human.
Dr. Lucie Low: Exactly.
Host: You have all these tests to see how it’s going to function and then this gives you another method, another check.
Dr. Lucie Low: Exactly.
Host: To say, yeah, this going to work in humans, but we haven’t necessarily poisoned anyone.
Dr. Lucie Low: Exactly.
Host: Yeah.
Dr. Lucie Low: And so, tissue chips are an incredible tool in that process. They’re not the be-all and the end-all. They’re not going to replace animals anytime soon we don’t think, but they could be an incredible tool in the drug development process. Another way that we can see that they could be really incredibly useful is in terms of disease modeling. So, if you look at the diseases that humans are faced with, cancers, genetic disorders, pathogenic infections, microbial infections, all these terrible kinds of things, every single person reacts differently to these cancers, to these infections, to these environmental exposures and so using tissue chips is a way to really understand in a very easily tightly controllable model system exactly what’s happening to your physiology or to your friend’s physiology or to your brother’s physiology in this in vitro system. So, it enables us to be able to predict population responses for example to different kinds of infections or if you can look at cancer populations or subpopulations if you have different kinds of genetically caused or genetically risk-driven cancers, then you can start using the tissue chips and modeling these in tissue chips to understand what exactly is it about this particular subpopulation that’s making them, that’s making their cancers act in a particular way towards a particular drug or what kind of particular drug might be more useful in this population than in this population, or what kind of cancer drug might cure the cancer in this population, but kill everyone in a different population?
So, the ways that you can use these chips to model disease and to understand the pathogenetic causes and all of the associated stuff that goes along with disease mechanisms in a chip, it means you just can’t do that in animals. You just can’t do that in 2-dimensional systems and you also can’t do it in a human, because there are so many other variables in humans that it’s a whole different can of worms to try and understand.
Host: Yeah. It sounds so, from what you’re describing, it sounds like this is very much in place. This is a product that’s being used right now for all of these different tests. Is that right?
Dr. Lucie Low: So, there’s a spectrum of answers to that.
Host: Okay. Okay.
Dr. Lucie Low: Tissue chips have been around for about a decade or so, but it’s only really in the last 5 or 6 years that there’s this really broad diversity of chips that have come to be created and developed.
Host: I see.
Dr. Lucie Low: And that’s partly due to a lot of NIH funding, so funding from the U.S. Government, funding from other governments around the world. There are a few commercially available tissue chips that different companies are selling. They’re modeling all kinds of different tissues, but at the moment it’s still quite early. It’s still pretty early in the bio, in this biotech stage. Its’ very exciting to see where it’s going to go, but there’s a lot of challenges that are still faced by the field that everyone as a community is trying to kind of crowdsource and workout some of the answers to.
Host: Yeah. It sounds like one of the things you were kind of going towards is more personalized medicine, more of that individual aspect of things. Understanding how these drugs or whatever may effect different populations.
Dr. Lucie Low: Yeah.
Host: Is that something that is being researched or is applied now?
Dr. Lucie Low: Absolutely. It’s one of those huge potential areas we see—
Host: Yeah.
Dr. Lucie Low: Could be, tissue chips could be massively helpful in. So, like I said, there’s lots of space for tissue chips in the toxicology world, all those kind of efficacy type stuff, but if you’re talking about precision medicine, that’s an early field in itself. So—
Host: Yeah.
Dr. Lucie Low: The medicine is definitely moving that way. It’s starting to understand that different genetics mean that different people are sensitive to different concentrations and different cocktails, combinations of drugs, but there’s that in itself there’s still such a huge area of research that, again, what we’re saying is that tissue chips could be an incredibly useful tool to model all of these and to pop into the toolbox.
Host: Yeah.
Dr. Lucie Low: To help answer these difficult questions.
Host: That’s actually why you’re in town today isn’t it? You’re talking with colleagues from around NASA or I guess other organizations as well?
Dr. Lucie Low: Yep exactly. I’m at a workshop today for precision medicine. I’m going to be talking this afternoon about tissue chips for disease modeling and precision medicine efforts.
Host: There you go. Well, thank you for stopping by.
Dr. Lucie Low: I’m delighted to be here.
Host: Alright, so we should probably dive into the fact that this is a capability that’s being tested right now, still a lot to figure out, but one of the things we’re looking at is using these in space, right? So, why, what do we need to know about how these are used in space? What is this going to help us understand?
Dr. Lucie Low: So, this is part of a really exciting program that where I work the National Center for Advancing Translational Sciences, is spearheading. We’ve partnered with CASIS which is the Center for Advancement of Science in Space and we have got together to send these tissue chips to, as you say, the International Space Station and we could not be more excited for a number of reasons. Microgravity has an incredibly disruptional effect on the human body in ways that we don’t necessarily fully understand and I know that you’ve had the 5-part series from the human research program talking about the different risks in space.
Host:Yeah.
Dr. Lucie Low: And so, a lot of those risks in space could actually potentially be modeled on tissue chips, so that’s the first thing is that these tissue chips could give really important information about disease pathology, understanding of microgravity effects in human tissues in in vitro systems, so that’s going to be useful for the space research field.
Host: Yeah.
Dr. Lucie Low: The space biomedical research field. But also, microgravity seems to cause changes in human physiology that actually directly translate to disease pathology here on earth. So, some of the fluid shift stuff that occurs up in microgravity is directly correlational to some different kinds of cardiovascular disease. There’s a higher incidence of kidney stones up in microgravity which we don’t really understand why. Kidney stones, big clinical problem.
Host: Yeah.
Dr. Lucie Low: Aging of the immune system or immunosenescence is seen as people get older down here on earth or they get exposed to more kinds of different viruses and colds and bacteria, their immune system responds appropriately or inappropriately and there’s been anecdotal evidence and some evidence of how T-cells for example, respond differently to microgravity in space and I think Dr. Brian Crucian was actually talking about that one on one of your previous podcasts.
Host:Yeah.
Dr. Lucie Low: So, there’s all these changes that happen up in microgravity that are really interesting and important and potentially very informative for human disease here on earth. And so, that’s what we’re using these tissue chips for in space is that we can model things that might take months or years to occur down here on earth if you’re looking at sarcopenia which is muscle loss or osteoporosis which is loss of bone density which is a huge issue for astronauts in space. We can model something that might take 10 or 15 years on earth to become even clinically relevant in a couple of weeks up in microgravity.
Host: Whoa.
Dr. Lucie Low: So, we are able to really try and start understanding disease pathologies and uncovering disease pathologies in a very accelerated way that we couldn’t do down here on earth.
Host: How is that? How is the timeline accelerated with microgravity?
Dr. Lucie Low: Well, that’s what we don’t understand.
Host: Whoa.
Dr. Lucie Low: So, that’s why it’s of interest both for us as researchers for human health here on earth, because we want to understand what is that causes osteoporosis? Is it genetic, is it environmental, what is it?
Host:Yeah.
Dr. Lucie Low: Up in space, there has to be a huge environmental aspect to it. So, what is the actual biological mechanisms and molecular biology underpinning that loss of bone density up on a station that is so fast? Could we potentially uncover new molecules that tissues respond to up in space that mean that it gives us potential new therapeutic targets to target osteoporosis here on earth? Could it give us insight into genetic mechanisms and genetic predispositions? So, we’re really looking to understand new things by being able to utilize the microgravity up on station.
Host: Wow. And this kind of goes back to your point of how small they are, right? This is a huge consideration for sending things up to space?
Dr. Lucie Low: Yep.
Host: Is mass is also a consideration when you’re sending things in a cargo vehicle. So, of you can send all of these chips with all of these different organs and functions—
Dr. Lucie Low: Yep.
Host: Altogether. That will give you some time.
Dr. Lucie Low: Yeah.
Host: And some I guess flexibility with what you can accomplish.
Dr. Lucie Low: Yep. And so, a key point that you just raised there is how the chips are small.
Host: Yeah.
Dr. Lucie Low: And that’s absolutely true. But if you look at the pumps and the computational needs that are needed to supply these chips with their microfluidic channels, with all of their plasma and all of their takeaway, all of their effluent that comes out the chip, then all of a sudden your teeny-tiny chip could need something to support it that’s the size of your kitchen refrigerator. So, one of the key challenges that our investigators have to face and that we’re really excited to be partnering with CASIS and with NASA to achieve is forcing our teams to make their teeny-tiny chips with their big refrigerator size support units. Put all their teeny-tiny chips into something the size of a shoebox.
Host: Whoa.
Dr. Lucie Low: Because that’s what’s going to fit on a rocket that can then be taken up to station and just be plugged and played literally like a Lego piece, just plug it in and play it. So, right now, a lot of the chips that are created and designed here on earth are quite bespoke, they’re quite artisanal, and so they’re developed by each individual lab and each individual researcher, but it’s very hard for them to translate that to a broader audience, because the specialty that’s needed to create and seed and get these chips functional is very specific and specialized and we’ve had the term a “Chip Whisperer” being thrown around because it can be quite complicated. You need really transdisciplinary experience and understanding to be able to get some of these chips to function. So, that’s another one of the challenges with the Chips in Space Program, is that our chips have to become what has been described by various NASA astronauts as “pilot proof.” [laughter] So, it has to be able for someone as stupid as an astronaut.
Host: Oh, okay.
Dr. Lucie Low: To be able to put— their words not ours, their words. [laughter] But it has to be simple enough and turnkey enough that they can take it out of the capsule that’s just arrived.
Host: Yeah.
Dr. Lucie Low: They can plug it into the systems on station, they can turn a valve, they can do this, they can do that, and it doesn’t require specialized scientific knowledge to be able to do that.
Host: Yeah.
Dr. Lucie Low: And so the ability to be able to create systems that do that mean that down here on earth we suddenly have this tool that can model of all of this cool biological stuff, all of this cool technical stuff, but it can be sent anywhere on the planet.
Host: Yeah. Wow. So, that’s funny what you said about the astronauts, I was laughing just because it’s mainly because they have so much to do, right? So, it’s like understanding this complex process is going to take more time and energy, the more simple you can make it.
Dr. Lucie Low: Yeah. Absolutely.
Host: The more easier the execution, the more people that can get their hands on it, but it sounds like that’s translatable to even just the process on earth.
Dr. Lucie Low: Exactly.
Host: You get these giant refrigerator size things down to a shoebox, if you get people that can go in and flip a couple of switches, read a manual, and then they’re good to go.
Dr. Lucie Low: Exactly.
Host: That makes the whole process a lot faster and easier.
Dr. Lucie Low: Exactly. And it takes it from a large complicated process that requires a lot of specialist need to something that any lab on the planet could have and any summer high school student could potentially be able to go in and actually run experiments in this way.
Host: So, you were hinting at some of the challenges of manufacturing tissue chips before, so what are those challenges? It sounds like you were talking about cross-disciplinary understanding of how the whole thing works. What are some of the hardest parts about creating these things?
Dr. Lucie Low: So, that’s a great question and I’ll preface this by saying that science is hard. It’s complicated. It’s messy. Things don’t work. It’s just a repeated iteration of failure and trying to get better. So, one of the key things about understanding tissue chips and their development is just how, like I said, transdisciplinary it is. You have technical challenges. You have biological challenges. If you’re talking about technical challenges, and I’ll just refer to the design of them here on earth because the space stuff is a whole different ballgame, but if you talk about technical challenges you have to think about what materials is your chip going to be made of? Is it going to be made of a kind of plastic that absorbs lots of different kinds of drugs or, but that you see through with a microscope, or is going to be made out of something else that is not so optically clear, so you might be able to see that the cells are doing in real-time instead? So, there are always tradeoffs related to the design of your chip based on what questions you want to ask of it. You might have to think about how you’re going to connect multiple different organ systems. So, we might not see bubbles as a potentially big problem if you’re talking about bubbles in tubes or piping, but if you’re talking about microfluidics, bubbles are death.
Host: Oh.
Dr. Lucie Low: Bubbles will kill your system, because they’re microfluidics can’t pump and your cells will die. If you’re talking about how to link different systems you have to start thinking about how are you going to maintain sterility. So, your cell culture in each of your systems can be quite different. So, how are you going to link them to make sure that when you plug that next little pipe in you don’t pick-up all the dirt and all the crud that’s on the desktop surrounding you that you’re plugging it into? So, there’s all these issues of sterility. If you’re talking about populating your chips, some of the biological challenges, cell sourcing is a huge issue in the field right now. You can buy commercially available cell sources for numbers of, many, many different kinds of cells, but you might get differences in the batches. You might get differences in the media that you need to get them to grow. It might take you 9 months to actually be able to get the kinds of mature cells that you need before you can even start using them. So, you’ve got issues with that. If you’re looking at, as I referred to earlier, induced pluripotent stem cells or IPS-derived cells, that in itself is a whole massive field of research in biology that’s only really been around for less than a decade.
It’s a huge exciting, massively, interesting field with so much potential, but it’s very early days. So, right now if depending on the tissue that you’re looking at, if you take skin cells or a punch biopsy or any other kinds of cells from a human donor, and you try and make them into a different kind of cell through different kinds of cell differentiation protocols, then there’s not necessarily any guarantee that what you’re going to get is what you are actually looking for. So, there’s all different kinds of issues with the protocols. There’s different kinds of issues with how mature the cells are. We talked about cardiomyocytes earlier on, if you take or if you try and derive IPS-derived cardiomyocytes from human donors from skin cells or whatever, you get a very young phenotype and phenotype is the word we use for, basically how it looks. So, you have you genotype which is what the genes are inside it and the phenotype which is how it comes out at the end. And so, you can get a very immature phenotype that might be equivalent to almost a fetus or a 2-month-old baby which when you’re trying to compare that to how that is relevant to the 50-year-old cardiovascular patient that they came from, then there’s clearly a disconnect.
Host: Yes.
Dr. Lucie Low: So, there’s a lot of work that’s going on in that field to look at cell sourcing.
Host: Yeah.
Dr. Lucie Low: Looking at the immune response; every single part of your body, every single organ in your system has different kinds of cells that would have a different kind of immune response very much within their system and it’s based on your experience. I talked about immunosenescence. It’s based on whether or not you had chickenpox as a child or whether or not you had a measles vaccine, all of this kind of stuff. Modeling that on a chip in this in vitro system can be incredibly challenging, because we still don’t understand in a full human system or animal systems, how all of those integrated organs might work together to give an either innate or adaptive immune response.
Host: Wow. It goes back to your opening kind of comment that science is hard.
Dr. Lucie Low: It’s really hard.
Host: Yeah. So, it’s not this plug-in and run sort of phenomenon that we’re requesting and this is going to be the challenging part.
Dr. Lucie Low: It depends on the system. There are some that are plug and play. There are some liver systems. There are kidney systems. Kidney proximal tubules that are complicated, but are relatively well-validated in a sense that they can be replicated in a number of different laboratories, they can be replicated with relatively standardized cell lines and so then you’re starting to get to the stage where you’re getting a product that is much more useful for the broader community, but it really depends on the chip, it depends on the system, it depends on the organ.
Host: Yeah.
Dr. Lucie Low: There are so many variables and so it’s an incredibly broad spectrum of where we are and where we’re going.
Host: Which is why it’s not a replace everything else now. We’re just doing tissue chips. It’s just another.
Dr. Lucie Low: Exactly.
Host: Yeah. Okay.
Dr. Lucie Low: So, certainly within the field we have a lot of controversy and banter and back and forth amongst our investigators and about people who might be end users how useful are these systems going to be? What kind of questions can we ask? And those are really great questions that everyone is involved in, because this is the evolution of a whole new biotech.
Host: Yeah.
Dr. Lucie Low: And it’s going to have multiple different uses on so many different levels and so everything we do we’re asking about why are we doing this? Why is this important?
Host: Yeah. Do you have an example that you can recall of something that you were testing with other models and then came to the tissue chips and said, “Oh, this is kind of surprising” or something that the tissue chips maybe revealed that wasn’t apparent before?
Dr. Lucie Low: And because the liver is the organ that does all of the drug metabolism and then spits it out to all the different organs.
Host: Yeah.
Dr. Lucie Low: A lot of what is incredibly important in drug development is the actual drug metabolism. And so, this is where what we call PKPD which is pharmacokinetic and pharmacodynamic modeling and various other kinds of modeling come into play, because if you can link tissue chips together, get integrated organ systems which we talked a little bit about some of the challenges.
Host: Yes.
Dr. Lucie Low: Then you can start understanding how sequential metabolism might happen for example in the liver, in the human. You can understand how you might take a drug through the mouth, some of your saliva enzymes might change how it’s broken down. You can run it through the gut and then see how the different kinds of gut acids might be effecting the different metabolites, send it to the liver, see what kinds of bioactive metabolites might come out of it, send it to the kidney and see which types of molecules might get stuck in your kidney. They might be nephrotoxic.
Host: Yeah.
Dr. Lucie Low: Or what kinds of metabolites might pass up and get passed through, for example, your blood brain barrier. Now, if you suddenly got active metabolites or something passing through your blood brain barrier, then you have a whole different world of hurt, because all of a sudden you’re bringing the brain into the equation as well and so you could be disrupting so many different systems within your body without realizing and that’s something that animal studies can’t necessarily replicate. Whereas, if you’re very targeted in how you link tissue chips and look at what you’re the outcomes that you’re getting from each chip and what’s being sent on and you can be very specific in looking at off-target side effects for example.
Host: Yeah. This goes back to your kind of statement about how it’s kind of progressing and evolving as we go on.
Dr. Lucie Low: Yes, exactly.
Host: And kind of linking all these tissue chips to understand, you know, you’re talking about tissues, talking about organs on chips, but how they’re connected and resembling the human body.
Dr. Lucie Low: Yes, human on a chip.
Host: And how everything effects everything.
Dr. Lucie Low: Exactly.
Host: Because honestly, you know, you take, you take like a I don’t know an antacid whenever your stomach is upset, but how is it affecting other things.
Dr. Lucie Low: Yep.
Host: You know? Just questions like that that you might not understand.
Dr. Lucie Low: Yeah.
Host: Or like how, how you take like a I don’t know antihistamine after you get like a bug bite and.
Dr. Lucie Low: Yeah.
Host: Somehow it disappears. I don’t know. This is all foreign to me, because I’m not like a doctor. I’m sure you’re like, “Oh, yeah that’s very simple”, but.
Dr. Lucie Low: Absolutely not. Nothing about this is simple.
Host: Oh, okay.
Dr. Lucie Low: Humans are not simple. [laughter]
Host: That’s why we need—
Dr. Lucie Low: We may think they are.
Host: Well, some people I know are simple, but—
Dr. Lucie Low: Their systems are pretty complex, and so we’re trying to mimic some of that complexity in these tools.
Host: Okay. So, why don’t we kind of revisit the tissue chips and just kind of go back to sort of the history, the inception.
Dr. Lucie Low: Okay.
Host: Of this. Do you know where it started? How it kind of evolved, because the idea of putting something on a chip just seems so like a.
Dr. Lucie Low: Yeah.
Host: A human function on a little device.
Dr. Lucie Low: Yeah.
Host: It just seems so foreign.
Dr. Lucie Low: Yeah.
Host: So, where did this all come about?
Dr. Lucie Low: So, so what is that phrase? Is it necessity is the driver of innovation or something like that?
Host: It’s beautiful enough as it is, yeah.
Dr. Lucie Low: So, so there’s been this huge push like I mentioned in drug development. There’s been this big disconnect between humans and animals. There’s been a big disconnect between 2-dimentional cell dishes and more complicated model systems and there’s this huge attrition rate in the development of new drugs. And so, early on about 10-15 years ago, the NIH, National Institutes of Health, got together with the FDA, the Food and Drug Administration, and they said “Hey, we have these problems. We need new tools. We need new ways to try and advance regulatory science and that was literally the name of the program was Advancing Regulatory Science. And so, they had a bunch of different applications that came in and one of the applications that came into that program was what, was for what was called the Development and Design of a Heart-Lung Micromachine, and this was if you like the original lung on a chip. This was a very elegant and quite simple, but still very effective design where they, the team actually designed the lung alveolus on a chip.
They designed a system where they had lung epithelial cells on one side and other kinds of cells on the other side and then they had a membrane between them which was, which they could if they applied vacuum forces down the side of this chip, they could cause the membrane to stretch and expand and contract, expand and contract.
Host: Just like the lung.
Dr. Lucie Low: Just like your lung, exactly. So, they were mimicking these biological forces to these cells on both sides of the membrane as would be seen in your lung alveolus, and so they were able to see using these different kinds of cells what effects the different kinds of drugs had on the system. They could look at bacterial infections and see how bacteria can pass through the system. They could look at things like nanoparticles, cigarette smoke, all kinds of different things that might affect our lungs and they could look in this little in vitro tool. And so, since then the premise of that was it was one of those things where if it was a good idea, someone’s going to come up with it anyway, but it was definitely there was a lot of interest at the same time and so as a result, NIH then decided to get together with DARPA, the Defense Advanced Research Projects Agency, and they were going to co-fund two different programs which had slightly different, slightly different aims but that would run concurrent with each other to fund the development of these tissue chips. And so, NIH funded a 5-year program which was for tissue chips for drug screening and DARPA ran a program which was to create a human body on a chip. So, DARPA wanted 10 different organ systems represented in one machine that you could plug-in and then do all this stuff. So, NIH and DARPA they had their same aim, slightly different goals.
Host: Yeah.
Dr. Lucie Low: And, but faced a lot of challenges, similar challenges along the way. So, those 5-year programs ran and they ended in 2017, and DARPA said hey this was awesome. You know, take it and go, like you guys did an awesome job, like we want to see what you guys come up with now. So, NIH is continuing to fund that and we’re now running a program called Tissue Chips for Disease Modeling and Efficacy Testing. We have the Tissue Chips in Space Program.
Host: Right.
Dr. Lucie Low: We have a Tissue Chip Testing Centers Program. So, we have a number of different programs that are not coming through to support the development of these chips in different ways and see where we can go and what we can do with this technology.
Host: Okay. So, let’s focus on the Tissue Chips in Space part. So, what’s the plan there? When are going to start ramping up and sending these?
Dr. Lucie Low: Well, so the first nail-biting launches begin in November.
Host: Okay.
Dr. Lucie Low: This year.
Host: Oh, wow.
Dr. Lucie Low: So, November 2018. So, we have our first teams getting ready to the decamp down to Kennedy Space Center.
Host: Okay.
Dr. Lucie Low: And they’re going to be setting their labs up there and getting their chips ready to launch. So, this was a 4-year program that began last year and now we have our teams getting ready to launch. They’re going to send two missions, two flights and the second flight is going to be building on what they learned from the first flight, both technical and biological.
Host: Okay.
Dr. Lucie Low: So, we have 5 teams funded through that and all of the information is on the NCATS website, but we also then partnered with NIBIB which is another institute for biomedical imaging and bioengineering at NIH. So, we partnered with them and we’ve, we reissued this program. We said, “Hey guys this is so great. We want to, you know, want to give you some more money. What else you got?” So, we’ve got another few projects that have just been funded through that and that’s going to be being announced very shortly. And so, those guys will be flying two years from now and then another two years from then.
Host: Wow. Okay, so I like that idea of building. So, you’re just the idea is find out what’s going to happen to these things in space, right? You guys will either they’re being sent and designed and tested, but then after you learn, to send more stuff up.
Dr. Lucie Low: Yes.
Host: So, is a lot of it the biological science or is some of it the systems themselves in making sure that shoebox thing is going to work. Maybe a little bit of both?
Dr. Lucie Low: It’s absolutely it’s both. So, say you’re looking at a system that is modeling the blood brain barrier, and you’ve gone from having one chip with a refrigerator size support mechanism to 12 chips in something the size of a shoebox and we do have a team that’s been doing that, then all of a sudden they have 12 times the number of things that could potentially go wrong with their pumping mechanisms. On, in a shoebox that’s going to be packed into a launch vehicle, sit on a launch pad for a while, and then rumbled around and then gets shot up into space at a high speed.
Host: Yeah.
Dr. Lucie Low: So, we don’t know what’s going to happen in that circumstance. We can plan and mitigate for as much as possible, as NASA does with everything they do that they’re sending to space, and we can get out guys to drop their chips from the tops of their buildings and see how they shatter or see if their cells detach from the walls of the chip inside the chip when they do that. So, we can make them run controls on hyper-gravity. We can make them run controls on microgravity. We can make them get there great-aunt Nellie who has never touched a petri dish or a pippete in her life to try and use the system and see just how pilot proof this system might be.
Host: Yeah.
Dr. Lucie Low: So, we can get our guys to do as many experiments on earth as they can to try to work out what could go wrong.
Host: Yeah.
Dr. Lucie Low: But until they do it, we don’t know.
Host: Okay.
Dr. Lucie Low: And then the key idea is that from the first flight that they do, the science that they’re going to be looking at is going to say oh, hey here’s something here that we haven’t seen before that we think is a result of microgravity and we’re going to have to do a bunch of different controls to make sure that it’s microgravity that’s actually causing that change, say and how leaky the blood brain barrier might be, but then we can take that result from the first flight and we can say well if we see that there’s this change in the blood brain barrier, we’re pretty sure it’s due to microgravity and we’ve got one more flight. Do we have any potential drugs for this kind of thing? Or is there a potential intervention? Or is there a potential disease that this might be modeling? Then you can investigate that with the second flight in an applied manner. So, that’s why we have these two flights. So, you could almost say the first flight as a practice.
Host: Yeah.
Dr. Lucie Low: It’s absolutely not. It’s incredibly scientifically rigorous, but it’s going to tell us what is actually going on so that we can then apply the results from that to maybe get new therapeutics, new disease mechanisms, new understanding of what’s going on in your body by shooting you up to space.
Host: Huh. Could you use the tissue chips as, I’m trying to think of how this works; can you use them in space kind of understand, you know, just kind of run it, understand what’s going on and then bring it down to earth, plug it again and run some, I don’t know, new drugs and see if it has some sort of effect? Is that something that something that is possible?
Dr. Lucie Low: So, yeah. Now you’re thinking like our teams have been thinking which is great.
Host: Alright.
Dr. Lucie Low: So, there’s so many different things you can do.
Host: Okay.
Dr. Lucie Low: So, some of our teams are sending the tissues up and they’re freezing them straight after they get to microgravity because they want to see what the effects of hyper-gravity were at launch.
Host: Okay. Oh.
Dr. Lucie Low: The stresses associated with a launch. Then they’ll have out of that cohort they’ll have some chips that they don’t freeze and they’ll sit in microgravity and bubble around for a while and do their thing and then they’ll freeze them.
Host: Okay.
Dr. Lucie Low: And then we have other teams that are sending their chips up to space and we have one team which is doing some really cool work looking at terminal differentiation of T-cells, so looking at the immune response and how microgravity effects it and so what’s very exciting with this project is that they’re going to be taking the chips up to space, they’re going to be able to see what effect launch has, what effect microgravity has, but then they’re also going to be bringing their chips back down to earth with the cells still buzzing and doing their thing. So, then they’re going to be able to see what effect the return to standard gravity has on their systems and whether it reverses the changes that they’ve seen through microgravity. So, that is going to tell you exactly what space flight associated changes there are when this particular immune response, for example, and how it can revert back to normal back here on earth, because that’s also something that a lot of the astronauts say, is that they come back down and those changes reverse after a few weeks or months.
Host: Right. That is fascinating. That whole process can be done with the tissue chips. That’s insane.
Dr. Lucie Low: Yeah. So, maybe one day we’ll be able to put astronauts on a chip and send them up either alongside the other astronauts or before they go after they’ve been and do personalized types stuff with astronaut data, with astronaut tissues.
Host: Wow. So, that’s the future then? There you’re talking about more personalized chips maybe even more functions on a single chip? Is that some of the future stuff you’re looking at?
Dr. Lucie Low: Yeah, yeah potentially.
Host: Wow.
Dr. Lucie Low: Yeah. So, some of the things that we can look at on the chips.
Host:Yeah.
Dr. Lucie Low: There can be a really broad range of outcomes you’re talking about that different kinds of things you want to look at.
Host: Sure.
Dr. Lucie Low: You can, some of the chips are see-through. So, you can put them under a microscope and see what’s going on in real-time.
Host: Yeah.
Dr. Lucie Low: Some of the chips have different kinds of electrodes embedded into them. So, if you’re looking at cardiac tissue or neural tissue, you can see how active the tissues actually are, if they’re buzzing, if they’re talking to each other with cardiac tissues you can see if their twitching. So, there’s already been some cardiomyocyte work that’s been done up on station where you can see that the actual cells where starting to twitch and contract like heart tissue would. If you’re looking at neural tissues, you can start looking at whether the synapses are doing their thing whether the nerve cells are talking to each other and so there’s lots of different kinds of analogs and outcomes that you can looking at that tell you what is going on in that tissue, sometimes in real-time in this system.
Host: Let’s talk about you Lucie, because this is super complicated and I keep thinking about that phrase where you said it’s multidisciplinary to really understand how these things work. What is your background and then who are you working with to all make this come together?
Dr. Lucie Low: So, I’m actually a neuroscientist by training.
Host: Really?
Dr. Lucie Low: So, I would like to say it’s the toughest of tough challenges in human research, but I’m sure that I’ll get shot down for saying that. So, I’m a neuroscientist by training, but I study the neuroscience of pain which is intensely personal but also intensely transdisciplinary. You have to be able to understand molecular biology. You have to be able to understand psychology and everything in between. So, I spent a number of years training as a neuroscientist, a pain neuroscientist and then I decided I wanted to step into the bioengineering biotech field and I was lucky enough to land this job.
Host: Yeah.
Dr. Lucie Low: Which is incredible and super exciting. And so now I work with bioengineers. I work with biologists from all different areas, because every single organ system that you have will have different specialists.
Host: Yeah.
Dr. Lucie Low: I work with materials engineers. I work with physicists. I work with electrical engineers and it’s, that’s why it’s so broad, you know.
Host: Yeah.
Dr. Lucie Low: Mathematicians, epidemiologists, computational theorists, all this kind of crazy stuff.
Host: Whoa. Okay, yeah. That’s much more broad than I was thinking. I was thinking more like, I don’t know, human sciences.
Dr. Lucie Low: No, it’s human sciences, it’s material sciences.
Host: Yeah.
Dr. Lucie Low: It’s physical sciences.
Host: Wow. Okay, yeah well that makes sense, right, because.
Dr. Lucie Low: Chemical sciences, must not forget them.
Host: Yeah, to understand how microgravity is, there’s a little bit of biology, but there’s a little bit of physics too.
Dr. Lucie Low: Yeah.
Host: There’s a little bit of math.
Dr. Lucie Low: Absolutely.
Host: Wow.
Dr. Lucie Low: Loads of math.
Host: This is very exciting. I keep thinking about the future and how this can be, how this can be kind of rolled out. You said it’s been evolving over time. There’s things we want to understand about how it’s going to work in space and what it can reveal about what’s happening to the human body. You know, you were talking about osteoporosis. You were talking about aging. There’s all these the immune system, all these effects that can happen from microgravity. Going forward, how do you imagine the future for tissue chips. You know, you were talking about astronauts on chips, you were, like for more functionality, more personalization. What’s the future for this?
Dr. Lucie Low: So, the short answer is all of those.
Host: Oh, wow.
Dr. Lucie Low: So, we like we said, we want to see these tools developed. We want to see them that they’re utility can be demonstrated and then we want to demonstrate to everyone that actually these tools are really helpful and you guys should try using them too. So, there’s avenues everywhere for that.
Host: Yeah.
Dr. Lucie Low: So, some of the areas of research and the stuff that we’re going to be focusing on in the future from NIH’s end, is moving towards precision medicine, personalized medicine type things. Looking at different kinds of subpopulations of patients, different demographics, sociodemographics, age demographics, gender, race, ethnicity, all of that good stuff and then also precision medicine. So, looking at for example rare disease populations. So, if you can take rare disease populations that might only have 5 or 10 people on the planet who are afflicted with a rare disease.
Host: Yeah.
Dr. Lucie Low: But we can get hold of some of their cells obviously with full informed consent and with them as, you know, involved in the process the whole way through.
Host: Sure.
Dr. Lucie Low: Then they can be involved in clinical trials on a chip. That means that they can have drugs tested in their systems on chip in vitro that doesn’t actually involve the risk that’s associated with rare disease patients for actually going through a clinical trial in person.
Host: That’s right.
Dr. Lucie Low: So, there’s loads of different kinds of applications we see there.
Host: Wow. And it sounds like more real-time, you know. There’s this the more chips you have, more manufacturing, more personalization.
Dr. Lucie Low: Yep.
Host: More efficiency, it just sounds like just an ever evolving sort of feel.
Dr. Lucie Low: Exactly. So, in all of the challenges that everyone faces, we’re all working together to try and overcome those and move forward as a field because there are key challenges for everyone, but the potential for these tools is really exciting.
Host: Yeah. That’s so wonderful. I kind of want to end with this is kind of backtracking a little bit thinking about the future, but just the process of working with the tissue chips in space and the relationships between NIH, between CASIS, between NASA, how does that all work to actually make this happen?
Dr. Lucie Low: So, a lot of it involves networking at conferences.
Host: There you go.
Dr. Lucie Low: Hanging out at the Tiki bars afterwards and talking freely. So.
Host: Yeah.
Dr. Lucie Low: Science is so collaborative especially with these transdisciplinary subjects. We really want to get people together. We want to be able to breakdown some of the barriers so that people feel comfortable talking to each other and if that involves sharing a pint after work, then I’m totally okay with that personally. I’m obviously not paid for with any kind of government funds. But yeah, our key point is that we, we’re all working for the same, towards the same goals.
Host: Right.
Dr. Lucie Low: From NASA’s perspective it might be to mitigate and understand the risks associated with long-term space flight.
Host: Right.
Dr. Lucie Low: For NIH’s end it’s understanding human health and biology and disease here on earth and how to make that better. But the point is that we both have things that we’re working on that overlap. There’s a lot of synergy there between what our end goals are and so we like to work with as many people as we can. My institute and NCATS in particular, everything we do is collaborative. Everything we do is designed to bring people in and say, “Hey you guys have got a great idea. What can we do with that? We’ve got this brilliant idea. We’ve have this expertise, let’s talk about this. Let’s see who we can try and work this out and crowdsource and move forward.”
Host: Yeah. And realizing that the execution of this experiment in space benefits all these different.
Dr. Lucie Low: Everyone.
Host: There you go.
Dr. Lucie Low: Yeah.
Host: Lucie, thank you so much for coming on and explaining this crazy straight-up sci-fi phenomenon of tissues on chips. I really appreciate you coming on today.
Dr. Lucie Low: It’s been wonderful. Thanks so much Gary.
[ Music ]
Host: Hey thanks for sticking around. So, today we talked with Dr. Lucie Low about these tissue chips and why we’re going to sending them up to space. So, they’re going to be launching on a cargo vehicle coming up here soon, so go to nasa.gov/ntv to find the latest launch schedule so you can watch them go to space live. We have exciting launches coming here over the next few months, so make sure to see what’s coming up here soon. Otherwise, you can go to nasa.gov/iss and you can actually see what we have on tissue chips so far and kind of see the updates as they come along, also on social media, Facebook, Twitter and Instagram we have the International Space Station accounts. Use the #AskNASA on your favorite platform to ask a question or submit an idea for the show even and suggest an episode coming up here in the future just to make sure to mention, Houston We Have a Podcast. This episode was recorded on September 25th, 2018 thanks to Alex Perryman, Pat Ryan, Bill Stafford, Steven Benowtiz, Rachel Berry, and Liz Warren and thanks again to Dr. Lucie Low for coming on the show.
Thanks to the Program Science Office for coming and filming today’s event. We’ll be back next week.